
Patient-centered design: where science and empathy merge styles-h2 text-white
<p><span class="medium"><br>September 19, 2022</span></p>
Patient-centered design: where science and empathy merge
<p><b>Deliver designs aimed at improved clinical outcomes, not just a “feel good” user interface.</b></p>
<p>Many in the life sciences industry have been talking about “patient-centric” healthcare solutions for years. But few of those solutions deserve the name. They often depend too much on trending technology and buzzwords, and too little on the needs of those providing care.</p> <p>Many so-called patient-centric solutions lack a rigorous, structured understanding of the disease being treated. Case in point: there are more than 400,000 health and wellness apps between the Apple and Google app stores, generating five million daily downloads — but <a href="https://www.economist.com/taxonomy/term/76969?page=93\&page%5Cu003d78=" target="_blank" rel="noopener noreferrer">users delete 95% of those apps within 24 hours of first downloading them</a>.</p> <p>Such efforts fail because they do not properly meet the needs of:</p> <ul> <li><b>Patients</b> for tangible value in terms of day-to-day disease management, their access to care, or how well treatments fit their lives and daily routines.<br> <br> </li> <li><b>Healthcare providers (HCPs)</b> for easily accessible data and meaningful insights.<br> <br> </li> <li><b>Caregivers</b> such as family or friends to actively help and support their loved ones through easy-to-use devices and applications, and instructions in their preferred language.<br> <br> </li> <li><b>Regulators </b>for clinically validated proof that the solution delivers the promised benefits, and that the patient’s data will be protected.</li> </ul> <p>Successful patient-centric designs require a deep understanding of diseases and what it’s like for everyone in the healthcare system to deal with them. They also require an understanding of the risk factors and preexisting conditions that can lead to an illness, and the clinically validated interventions that improve outcomes.</p> <p>Here are lessons we’ve learned about getting patient-centric design right, and the types of life-changing — and market-changing — innovations it can deliver.</p> <h4>Getting patient-centric design right</h4> <p>Effective patient-centric design begins with a “discovery phase,” starting with detailed ethnographic field research into the experiences and needs of patients and providers.</p> <p>A co-creation or design thinking workshop follows, employing cross-functional expertise to translate the research insights into tangible solutions. Next is a series of Sprints to iteratively design and develop solutions, with frequent feedback loops from patients and caregivers.</p> <p>Most importantly, to ensure solutions achieve desired outcomes, designers must have a deep understanding of the symptoms and effects of a disease and how it manifests. (Please see the diagram below.)</p>
#
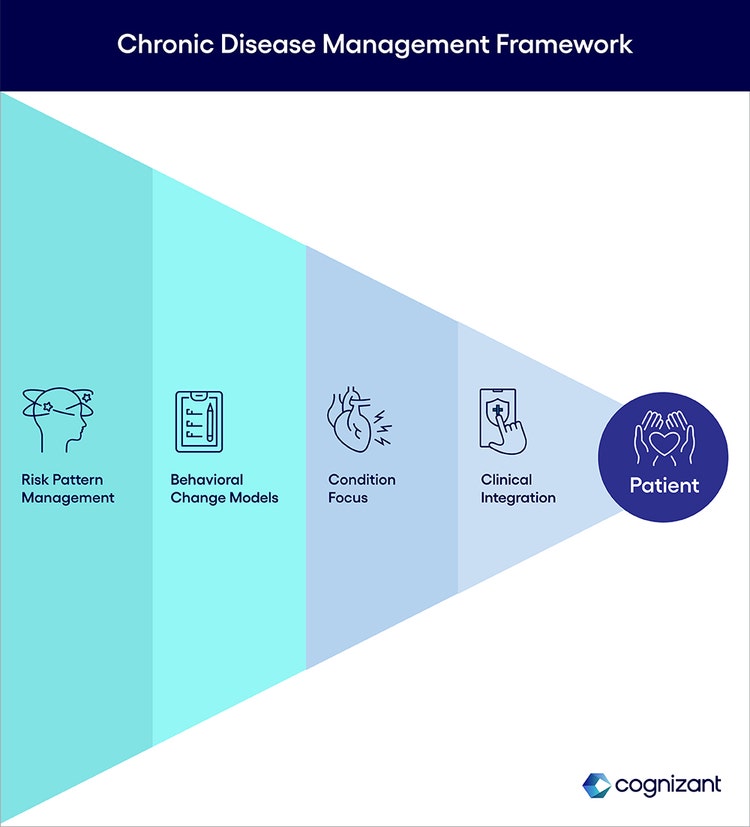
<p><span class="small">Figure 1</span></p> <p>An effective disease management framework comprises:</p> <ul> <li><b>Risk pattern management:</b> An understanding of a patient’s preexisting conditions or contributing behavioral patterns, not just their apparent symptoms. For congestive heart failure, for example, this might mean considering blood pressure levels, cholesterol levels, genetic predispositions, and the patient’s lifestyle such as whether they smoke and their sodium intake.<br> <br> </li> <li><b>Behavioral change models:</b> Frameworks that help patients overcome the human resistance to change. This might involve learning about their daily eating habits and providing ideas for simple heart healthy meals to nudge them to healthier eating in a culturally sensitive way.<br> <br> </li> <li><b>A focus on the specific condition:</b> Deep knowledge of the clinical definitions of a disease and how to treat it. This may require extensive research, including looking in academic journals or research papers to outline the biomarkers and physiological factors involved in a disease and then developing ways to measure or influence these factors through the digital solution.<br> <br> </li> <li><b>Clinical integration:</b> Assurance that all stakeholders have the information they need and can intervene as required as the patient’s needs change. This means, for example, making it easy for a patient to contact their doctor if their condition worsens, or to schedule a virtual appointment.</li> </ul> <h4>Tapping diverse skills</h4> <p>Combining these elements in innovative treatments requires skills not always found in traditional design teams. These include product design, digital health, technology and medical anthropology to understand how patients experience illnesses, as well as input from physicians, patients and researchers.</p> <p>Just as in Agile software development, the group should design in iterative Sprints, developing rapid prototypes that the group can quickly refine based on user feedback. Such efforts can move from initial exploratory work to testable proofs of concept within two to three months.</p> <h4>Brainstorming without fear</h4> <p>To that end, establish a judgement-free zone where any idea is welcome, even if it comes from other industries or would require substantial work to implement. Team leaders should not only state this explicitly but use exercises to encourage the widest range of input. These include “Crazy Eights” in which each participant has eight minutes to sketch eight big ideas for a digital healthcare solution as if there were no cost or technology constraints.</p> <p>We often find that, early in the process, medical or pharmacological experts who may be accustomed to a very structured clinical research approach face challenges accepting design thinking methodologies and exercises. Digital health leaders can overcome this resistance by articulating how these exercises can identify unmet needs and lead to the design of creative solutions. Often, we find the early skepticism about free-wheeling design thinking disappears and medical and pharmacological experts become much more enthusiastic as they see the creative solutions it delivers.</p> <h4>Scalability via digital components</h4> <p>To scale such solutions for a higher volume of patients and a wider variety of conditions, the team should create reusable digital components. These might include common user interface elements for patient- or doctor-facing applications, mechanisms to capture and store informed consent, pipelines to gather and normalize data from popular wearable health monitoring devices, and microservices to integrate electronic medical record systems.</p> <h4>Patient-centric design at work</h4> <p>We worked with a global biopharmaceutical provider client using this patient-centric design approach to help patients suffering from two diseases. The first was an inflammatory bowel disease (IBD) that causes severe bouts of long-lasting pain and frequent, unpredictable needs for a bathroom. The second was an acute, life-threatening condition that can strike cancer patients.</p> <p>Seeing the challenges IBD patients face with self-injection during treatment, the team developed a self-paced video application that lets them review directions for each step (such as cleaning the injection site) without touching their computer or digital device and thus keeping their hands clean to prevent infection. </p> <h4>Augmented reality & bathroom passes</h4> <p>Open-ended brainstorming also helped the team envision an augmented reality application that uses input from their phone camera to help them identify the proper injection site. A patient praised a key aspect of this feature, which helped remind him of the location of his last injection so he can avoid it next time. “It's eight weeks between [injections],” he explained. “Sometimes I had no idea where I put the last injection.”</p> <p>To ease patients’ isolation, the team envisioned a digital “bathroom passport” a patient could discreetly show at stores and other public places to gain access to otherwise inaccessible restrooms.</p> <h4>AI facilitates gastric insights</h4> <p>Yet another proposed application would use AI to identify ingredients in food from photos of their meals and correlating this information with their bathroom use to help them assess which foods trigger their symptoms. </p> <p>The use of AI to correlate foods and symptoms will help eliminate biases in reporting by patients, says one doctor. “If you like a food, you are less likely to associate it with your symptoms. If you hate a food, you're more likely to associate it with your symptoms. But with...the AI trends...you can exactly pinpoint where the problem is." </p> <h4>Cancer markers & smart water bottles</h4> <p>Our client took the same approach with the acute, life threatening condition for cancer patients, considering the needs of doctors as well as patients. Working with them, we envisioned an integrated risk assessment system to help doctors more easily and quickly estimate a patient’s risk of the condition by continually measuring a biomarker such as their potassium levels to assure they are properly monitored for it. We also proposed the use of smart water bottles to help physicians monitor whether at-risk patients were hydrating themselves adequately. </p> <p>The team’s in-field research with patients and understanding of their needs has brought new levels of passion and satisfaction to our work. True patient-centered design can drive previously impossible levels of care and competitive advantage. But it requires changing the mindset of the organization, fostering a culture of patient-centric innovation and a rigorous, science-based approach to solving problems faced by stakeholders across the healthcare ecosystem.</p> <p>Patient-centrism is too important to stint on either the science or human considerations. The patient-centric design/development process described above should ensure that solutions are continually tailored for the actual patient and their care team.</p> <p><i>To learn more visit the </i><a href="/content/cognizant-dot-com/us/en/industries/life-sciences-technology-solutions.html" target="_blank" rel="noopener noreferrer"><i>Life Sciences</i></a><i> section of our website or </i><a href="/content/cognizant-dot-com/us/en/about-cognizant/contact-us.html" target="_blank" rel="noopener noreferrer"><i>contact us</i></a><i>.</i></p> <p><i>This article was written by Bryan Hill and Vidya Viswanathan, Digital Health & Innovation Leaders in Cognizant’s Life Sciences practice.</i></p>

<p>We’re here to offer you practical and unique solutions to today’s most pressing technology challenges. Across industries and markets, get inspired today for success tomorrow.</p>